They let me out to play for a few days in Luanda, the Angolan capital... I never imagined a supermarket, sit-down toilet, newspaper, bed (NOT supplied by Guantanamo Bay Outfitters as i suspect my last one was), and hot shower could bring so much joy....
Photos below are of Mavinga and the projects there.
In order:
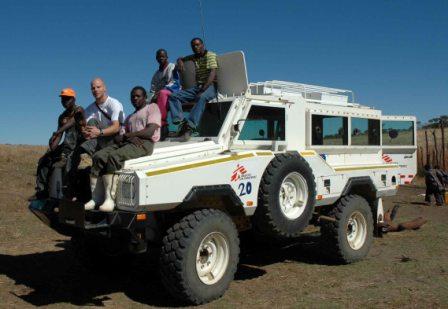
the water project, 2 typical scenes of the town here, a 'permanent' patient (an albino woman) with unfortunately common skin cancers who lives in a tent behind the hospital, myself and the rest of the exapt staff pretending to work c/o photoshop (this delighted our local staff to no end!), skyline at night, young girls at the river, 3 kids in the window of the shelled-out old school in town, old bomb in the new market, next 2 photos of patients in the malnutrition ward (mostly their families), me in my trendy new Mu-Mu, our anti-mine car, me in the cockpit of the charter flight out to Mavinga, one of the cooks in the hospital kitchen looking like a rock-star, adults ward at the hospital, fetching buckets of water at sunset with the cart, a Russian cargo plane drops off our supplies (after almost landing on our Co-ordinator - read below), high school in town, the two subjects of 'My Brothers Keeper' below...
Love to hear from home, wherever that may be to you.
Please put subject: damien brown